
Minimally Invasive Esophagectomy: A Better Surgical Option for Patients with Esophageal Cancer
-
In 2012, the American Cancer Society estimated the annual number of new esophageal cancers to be 17,460.
Surgical resection with radical lymph node dissection, usually performed after a patient receives either preoperative chemotherapy or chemoradiation, is regarded as the only curative option for resectable esophageal cancer.
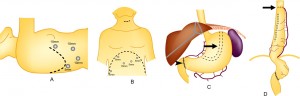
Surgical removal of the esophagus and reconstruction of the gastrointestinal tract, most commonly achieved by mobilizing the stomach in the abdomen and moving it into the chest to take the place of the resected esophagus and thereby restore a patient’s ability to eat, is a complex procedure. Although mortality rates have decreased over the years at surgical centers of excellence where this operation is performed more frequently, postoperative complications can still occur.
The most common postoperative complication is pneumonia (an infection in the lung). Recovery most commonly involves antibiotics and a prolonged hospital stay, but can result in additional days in the intensive care unit and even the need for mechanical ventilation. Traditional “open” esophagectomy, performed through two large incisions (one on the upper abdomen and one on right side of the chest), is associated with a significant likelihood of postoperative respiratory problems.
Initial attempts to minimize the impact of open esophagectomy surgery on a patient’s postoperative lung function focused on the use of open surgical techniques that eliminated the chest incision by substituting a small incision on the left side of the neck, the transhiatal esophagectomy (THE) operation. Instead of working through a large chest incision, the surgeon blindly frees up the esophagus in the chest by sticking one hand up into the chest through the abdominal incision and placing the fingers of the other hand as far down into the chest as possible through the small left neck incision. By eliminating the chest incision, lung function was improved but at the expense of being able to do a good lymph node dissection and removal of the cancer because the surgeon could not actually see inside the chest.
Beginning in the early nineties, some surgeons began to use minimally invasive surgical techniques to remove the esophagus. These techniques were similar to so-called laparoscopic surgery. Minimally invasive esophagectomy (MIE) used a video camera placed through a small incision (5-10 mm) to allow the surgeon to see inside the body. By using specially designed surgical instruments that he/she places though additional small incisions, the surgeon is able to perform the same operation as with open surgery, but without the large incisions. That means that the number of lymph nodes removed and the likelihood that all visualized cancer was removed (a complete resection) should be the same as open surgery and better than THE. Compared to open surgery, MIE should result in less impairment of pulmonary function in the postoperative period, as well as less overall pain and a quicker return to normal activity after this major operation.
The benefits of MIE compared to open esophagectomy were proven in a randomized trial conducted in the Netherlands and at other European medical centers. Patients with resectable esophageal cancer were assigned by chance to undergo esophagectomy though a traditional open technique or a minimally invasive technique (MIE). Patients were shown to have as equally successful rates of cancer resection with either approach. In addition, patients who underwent MIE had decreased pneumonias, decreased pain, went home sooner, and had improved quality of life following surgery. [Biere S, et al Minimally invasive versus open esophagectomy for patients with esophageal cancer: a multicentre, open-label, randomized controlled trial. Lancet 2012; 379: 1887–92)].
In summary, MIE, when performed at an experienced surgical center, is an equivalent cancer operation compared to open surgery and yet is associated with fewer pulmonary complications, a shorter length of stay, less postoperative pain and a better quality of life in the postoperative period.